
In an era of implantology in which the fashion for immediate implants is gaining popularity, it is important to mention the limitations that this type of procedure presents, since on many occasions it may seem like an optimal case but it really is not.
It is essential not only to review the scientific literature before accepting or not accepting techniques that make us leave our comfort zone, but to learn and revise the Biology that supports certain procedures which are supported by this superior entity and this language which is the one that makes us predictable above all else.
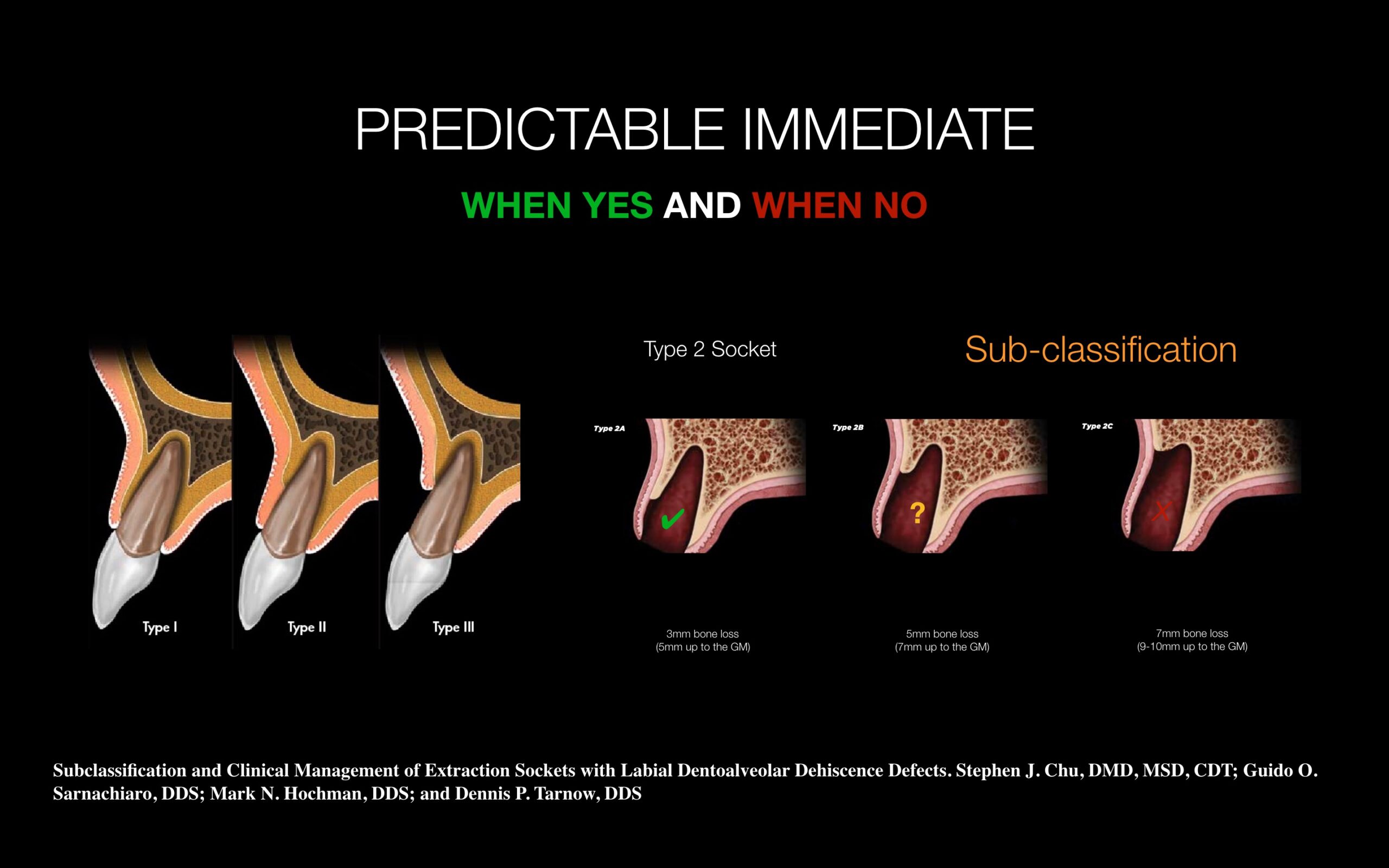
Years ago, the different types of post-extraction sockets (type I, II or III) indicated the anatomical limitation of the socket to be a candidate or not for the post-extraction implant procedure, especially taking into account the critical aesthetic profile and subsequent bone and gingival remodeling.
With active design implants and rapid osseointegration we are confusing paths since one thing is the versatility that our implant system can have for immediate placement after extraction and the other is the viability or not for the scenario to be optimal enough to regenerate / remodel / condition both hard and soft tissues after our placement.
Assuming that after implant placement “there is no way back”, or at least it is not what our patient expects, we must be firm when assessing whether our patient / implantation area is optimal for the predictable placement of our implant. That is why the studies published by Steve Chu, Dennis Tarnow and Cols specify that type II post-extraction socket are the most sensitive when deciding whether or not it is time to place the implant.
It is my obligation and interest to inform and train our future generations that not everything is valid, not everything can be sold and not everything is wonderful when it comes to learning a new technique, since one thing is to learn the technique and the other is to implement it in favorable cases.
Review the literature and use biology as a support to generate your own criteria when executing what we like the most, which is to rehabilitate our patients surgically and prosthetically.
Being predictable and trusting not only in our skilled hands but also our knowledge and learning management is paramount if we want to enjoy what we do.