
Dental Prosthesis represent the starting point at any Implant Restoration for proper dental implant planning.
This is the reason why even today we should have in mind that everything starts with the prosthetic guide regardless the multiple abutment types that we have available in the market which can angle & reposition the final insertion of the crown.
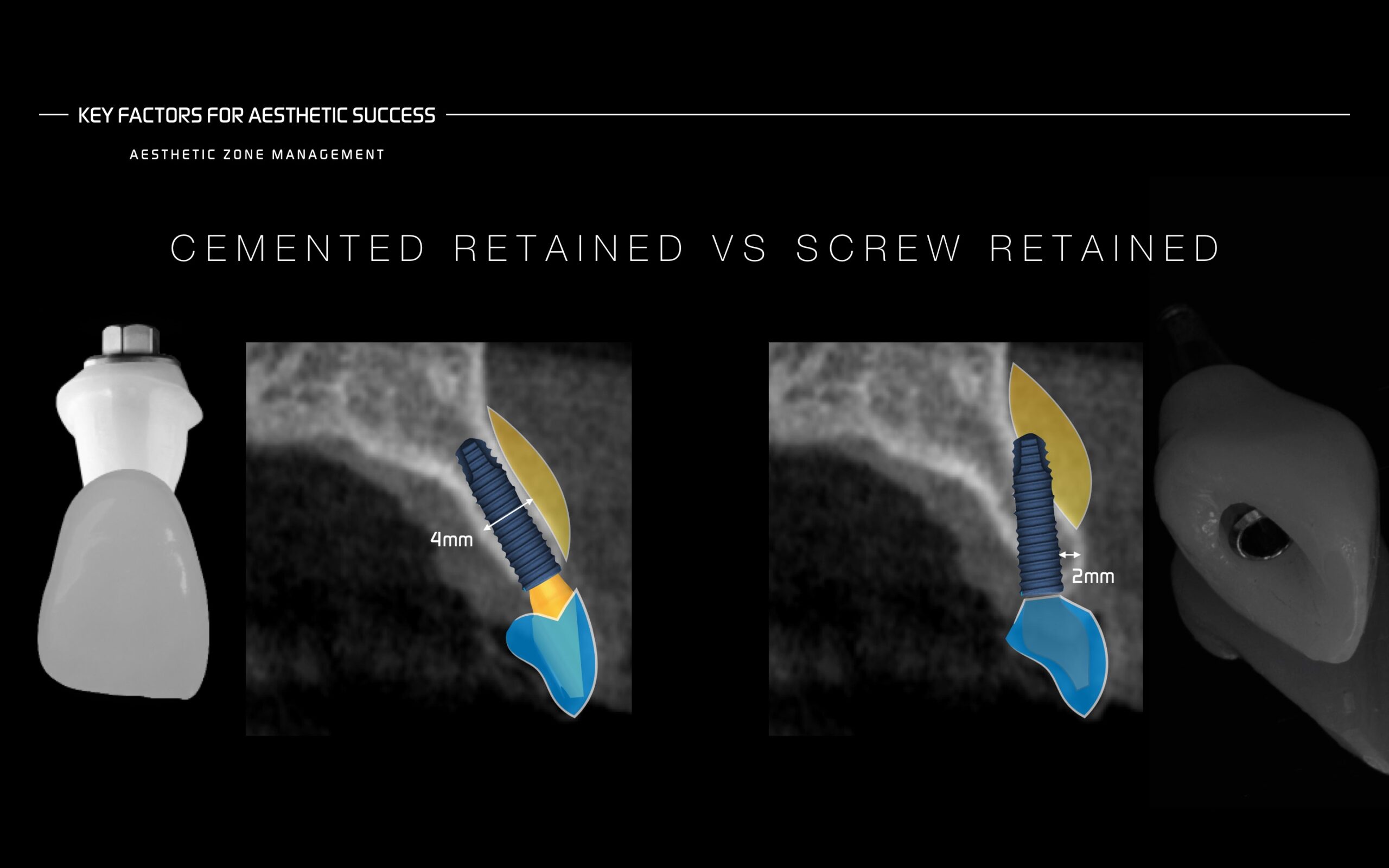
The truth is that many articles have been published comparing screw retained with cemented retained restorations and if we look at the literature the screw-retained implant-supported reconstructions have been found to pose less biological and technological complications.
Cemented retained restorations exhibit more biological complications addressed to the excess of cement, sometimes reduced by placing the implant at more coronal position or by using cement drainage holes which allow the release of cement as the crown is inserted.
Screw retained restorations complications could be addressed to screw loosening or fracture, implant fracture, microleakage by micromovement.
The solution resides on trying to reduce the impact on micro movement & micro leakage by treating the cause at distance by controlling occlusion as well as parafunctional habits and even blocking the excessive power of masseter muscle with Botox®. Locally by switching to cone morse connections or Morse taper connections we can reduce the micro-movement and micro leakage efficiently.
But the question resides on what if our customized abutments cannot overcorrect the initial implant position?
We must take pre-surgical decisions and understand that there is always a solution for every single case. Unless we use pure Guided Surgery and that step would be obligated in order to manufacture the final surgical guide.
Bone atrophy due to tooth extraction or abscence exhibits a ridge deficiency in horizontal and vertical aspects depending on the pattern of bone loss which sometimes shows proclined alveolar ridge shape.
By placing our implant in the proper position and leading to an apical fenestration, can this represent a risk for implant success? Is it recommended to graft over it? How much implant exposure would be reasonable not to graft?
A small fenestration should not be considered a big issue and sometimes could be left exposed but covering it with bone graft should be the first option in order to avoid problems down the road. That part of the implant is the less affected in terms of function as the occlusal forces dissipate along the implant.
In addition, providing more buccal bone facial to the implant by repositioning the implant more palatally brings two different benefits:
1-. We can provide a screw retained restoration even on a very proclined ridges.
2-. More buccal bone at the most coronal aspect of our implant is present thanks to this new implant position.