
The immediate implant placement after tooth extraction technique brings many benefits compared to traditional staged implant placement approach.
This is the reason why we should learn a predictable technique in order to be able to perform it, offer it to our patients and become different from the rest.
Advantages of this technique:
– The consequent bone loss is minimum since most of the times there is no periosteum reflection no flap release or elevation. The buccal plate is maintained and supported by particulate bone graft inside the gap from day 1.
– Asymptomatic from the patient experience and fast recovery time since there is no post op inflammatory effect.
– Reduction of surgical times since we are placing the implant the day of the extraction.
– Hard and soft tissue original architecture preservation by maintaining the original volumes and avoiding the buccal collapse addressed to tooth extraction alone.
– Papilla preservation height as long as you have adjacent teeth with intact inter proximal bone and proper attachment to the mentioned teeth as well as atraumatic extraction needs to be performed.
Important factors to take into account whenever we perform this technique:
1-. Proper radiological analysis with CBCT in order to visualize the bone volume and availability for the immediate implant placement to guarantee the minimum primary stability of our implant.
2-. Discard potential communications with maxillary sinus or floor of the sinus in close relationship of the teeth extracted with this areas or affected by apical cysts or chronic pathologies that might alter the real bone volume and even create a potential infiltration of particulate into this spaces.
As long as there is no communication after cyst removal, the implant can be placed ensuring the complete removal of granulomatous tissue.
3-. .Always try to keep the correct prosthetic guide.
4-. The lack of buccal plate along with soft tissue dehiscence or gingival recession would be a contraindication to perform this technique since the lack of periimplant soft tissue will expose the implant surface and a potential complication may develop.
In this case the staged approach is recommended to allow the re-epithelialization of the area and avoid soft tissue dehiscence.
5-. The tooth extraction needs to be performed atraumatically in order not to damage the supporting bone of the tooth. In case of buccal plate fracture we will determine whether to place the implant immediately or not depending on:
– Presence of gingival margin at the original position.
– Remaining bone available due to reduction to confirm implant primary stability at the proper position.
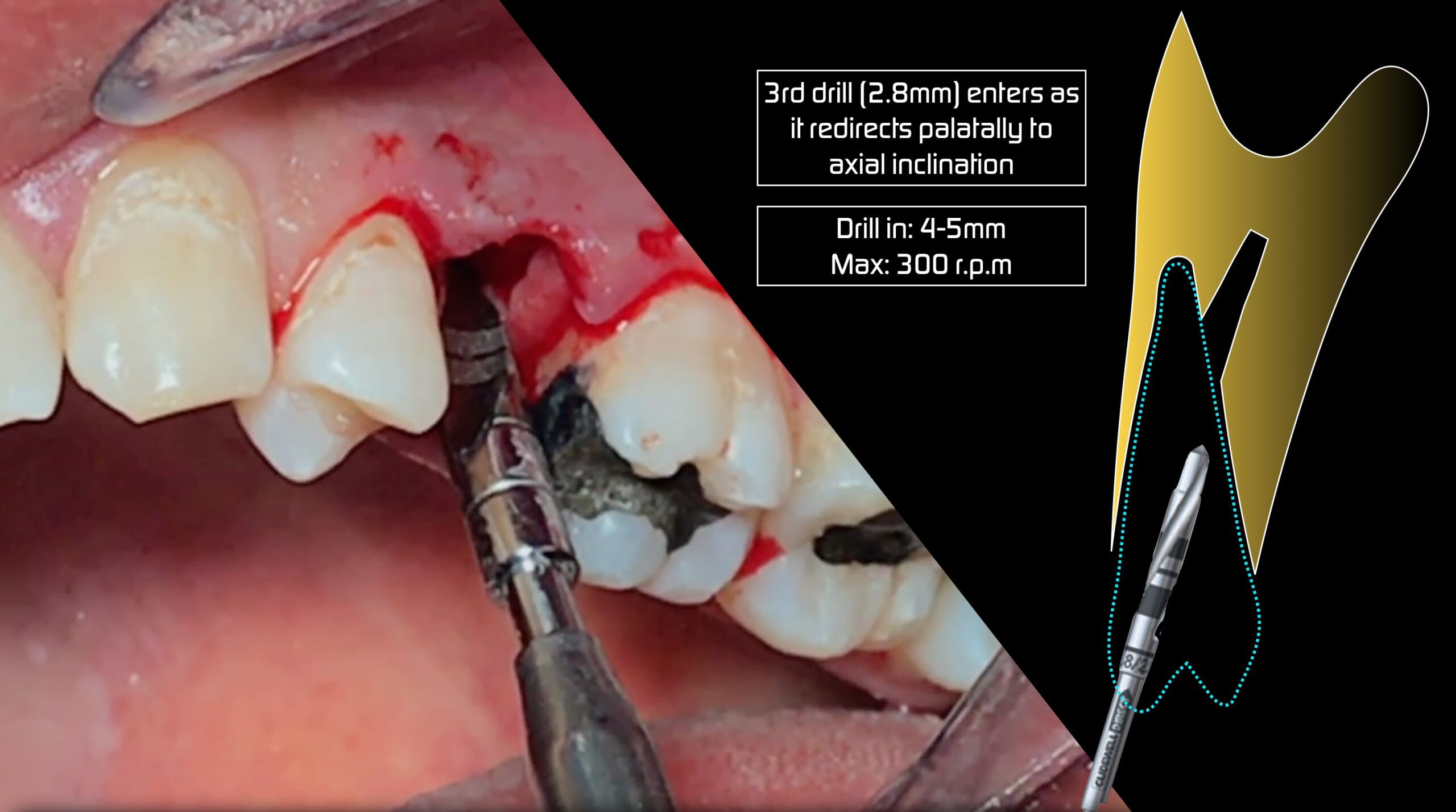
6-. During the implant insertion the references will be:
-Coronal reference: Buccal plate and never the lingual since the buccal plate is located mostly 2mm more apical than the palatal plate ( Masterclass: Immediate extraction & implant placement in posterior areas. M. Hürzeler ).
-Apical reference: Inferior alveolar nerve, Maxillary Sinus, Mandibular concavity and nasal floor.
7-. The drilling technique to guarantee the stability of our implant will depend on the bone density, drilling area, bone availability, etc…
8-. This technique can be performed along with immediate loading or using an expensive healing abutment to avoid extra tissue management since we are not disrupting the original position of the gingival margin.
Also the fact of blocking the gap with the crown or the abutment will keep the bone particles in place avoiding their release.
Learn the predictable protocol for this technique to reduce time, stress, increase predictability and avoid complications
Le agradezco la información que nos brinda