
The different biomaterials will follow a different biology so understanding the biological behavior will help us to understand the purpose and indication of each one of them.
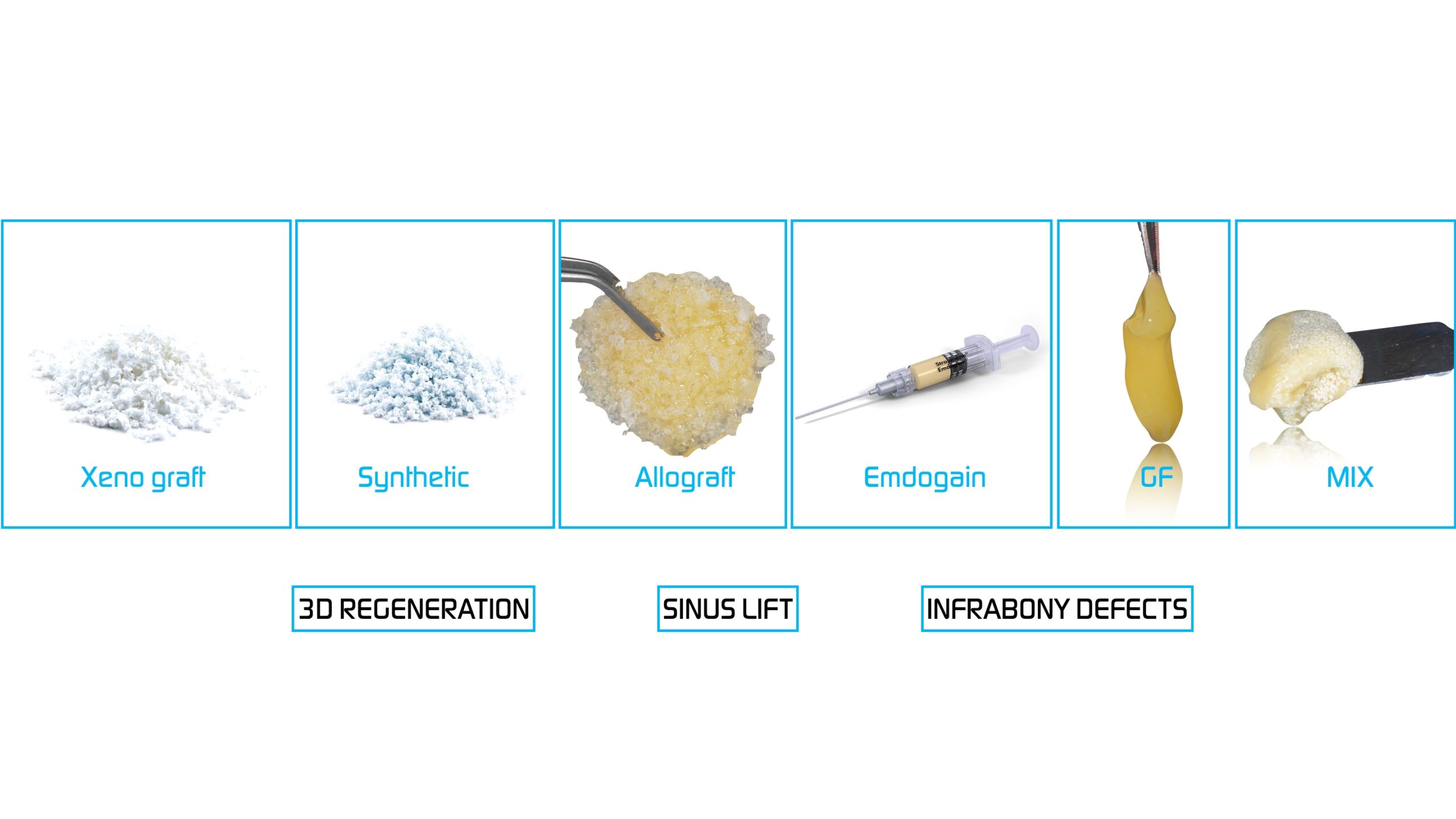
The most commonly used biomaterials are Xenograft, Autograft, Synthetic and Allograft among others.
1-. Xenograft: Good long term stability for bone volume maintenance but very slow vital bone turn over. Indicated in mild-moderate defects for GBR always covered by a membrane.
2-. Autograft: Gold Standard, the highest potential for bone regeneration and still pluripotential cells inside the graft but difficult harvesting a big piece of it unless we go to mandible ramus, chin, etc…
Indicated: Severe Atrophy or mixed with Xenograft on GBR procedures to increase the regenerative potential and vital bone turn over.
Keep in mind the high chances of bone graft shrinkage and mix it with Xenograft to compensate this issue.
Also one of the best for infra-bony defects in GTR procedures.
3-. Allograft: Great vital bone turn over and one of the best for Severe Defects when harvesting is not an option because of not enough training or not availability. 30-40% of it will disappear after integrating when vital bone turn over sets up.
4-. Synthetic Bone: BTCP+, CaP are becoming very popular in Regenerative procedures.
BTCP+(Beta Tri-Calcium Phosphate): Mild to moderate defects, infra-bony defects, socket preservation and Sinus Lift Procedures specially inside the sinus to avoid non vital bone into this space.
Calcium Phosphate: One of the best in bone regeneration by its osteo-inductive potential even at the soft tissue levels changing the biotype by improving the underlying bone.
5-. Emdogain: Not considered a Biomaterial but a Bioactive modifier with PDL regenerative properties by inducing the cementoblast proliferation and cement formation for new PDL growth. Indicated for GTR procedures.
Growth Factor Therapy: A biological Bioactive Modifier whose properties, promote the angiogenesis, increase the blood supply and improve the healing of hard and soft tissues.
The agglutinant properties over the particulate graft helps to integrate and stabilize the graft over the hosting bone.
The bacteriostatic effect avoids local infection at the areas exposed to potential dehiscence especially under the flap and incision line.
Non cooperative patients and heavy smokers would be candidates to be treated with additional GF therapy.